This tension has intensified as the sector has scaled. U.S. healthcare and pharma ad spending exceeded $30 billion in 2024, with pharma alone spending over $6 billion on DTC television that year. More money, more messages — and more ways to cross the line.
This article covers the core risks healthcare advertisers face: misleading claims, ethical violations targeting vulnerable patients, regulatory exposure across multiple agencies, and the specific hazards of digital and programmatic channels.
Key Takeaways
- Healthcare advertising reaches people who are ill, anxious, or desperate, which means ethical failures here cause real harm — not just reputational damage
- Misleading claims and outcome promises carry real clinical consequences, not just regulatory fines
- Fear-based messaging and privacy violations — including pixel tracking — erode patient trust and expose brands to legal liability
- Compliance spans four overlapping bodies: FDA, FTC, HIPAA, and state medical boards
- Digital channels introduce algorithmic restrictions, ad blocking, and brand-safety risks absent from traditional media
Why Healthcare Advertising Is Held to a Higher Standard
Before 1977, professional advertising was effectively prohibited in the U.S. A state bar in Arizona sanctioned two attorneys for publishing their fees in a newspaper ad. The Supreme Court struck that ban down in Bates v. State Bar of Arizona (1977), ruling 5-4 that truthful professional advertising was protected commercial speech.
That ruling opened the door for physicians, hospitals, and eventually pharmaceutical companies to advertise. But it didn't erase the underlying reason those restrictions existed.
The 1847 AMA Code described resorting to "public advertisements, private cards, or handbills" as "derogatory to the dignity of the profession." Those norms reflected something real: medical decisions are not like purchasing decisions.
The Core Tension
When someone buys a car based on an exaggerated ad claim, they're frustrated. When they choose a treatment based on one, they may be harmed. That asymmetry is why healthcare advertising faces a higher standard than consumer goods marketing:
- The audience is emotionally vulnerable — patients are often distressed, in pain, or frightened
- The product directly affects physical wellbeing — not lifestyle, not convenience
- Misinformation can delay or distort clinical decisions — with lasting consequences
A 2024 scoping review of DTC healthcare ethics found that 70% of reviewed publications raised questionable efficacy or quality concerns, 66% raised safety concerns, and 56% raised misleading advertising concerns.

Those numbers reflect why regulation followed. The AMA's current Code of Medical Ethics (Opinion 9.6.1) still restricts deceptive advertising, unjustified expectation-setting, and misrepresentation of qualifications. Truthful advertising is permitted. Manipulative advertising is not.
The Risk of Misleading and Unverified Claims
The most immediate risk in healthcare advertising is making claims that aren't substantiated. The FTC's Health Products Compliance Guidance is explicit: health-related claims must be truthful, not misleading, and supported by competent and reliable scientific evidence — which, for many benefit claims, means randomized controlled human clinical trials.
Outcome Promises and Testimonials
Ads that imply guaranteed results or specific cure rates are a direct regulatory target. The FTC's Endorsement Guides state that endorsers cannot be used to make claims the advertiser itself couldn't legally substantiate — and material connections must be disclosed clearly.
Patient testimonials showing exceptional recoveries carry particular risk. The core problem:
- Implying that an outlier outcome is typical violates FTC standards
- Undisclosed paid relationships between advertisers and endorsers constitute deceptive practice
- "Before and after" framing that omits context (diet, concurrent treatments) can mislead consumers
The "Specialist" Problem
Healthcare advertising regularly misuses credentialed language. Calling a provider an "expert," "specialist," or "best" carries legal weight when those are professionally or legally defined terms. The North Carolina Medical Board warns licensees against implying unusual skills or claiming board certification without current proof of certification by a recognized board. Misuse can constitute false advertising and trigger licensing board action.
Statistical Spin
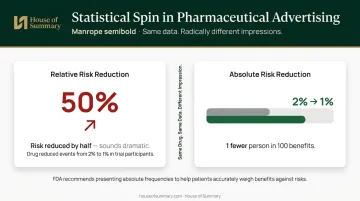
Relative risk framing is where technically accurate data becomes functionally deceptive. A 1999 study of 22 drug advertisements found that 11 reported clinical outcomes solely as relative risk reductions — a format that makes benefits appear larger without the context of baseline risk.
The FDA's December 2023 guidance warns that relative presentations can cause consumers to overestimate benefits or underestimate risks, and recommends presenting absolute frequencies instead.
A drug that reduces an event rate from 2% to 1% has a 50% relative risk reduction but a 1 percentage point absolute reduction. Both are technically accurate. Without the absolute figure, patients have no way to weigh that benefit against a drug's side effect profile.
Ethical Pitfalls: Exploiting Vulnerability and Eroding Trust
Healthcare advertisers often reach people at their lowest — someone newly diagnosed, a parent searching for answers at 2am, someone in the grip of addiction looking for help. That creates a power imbalance that advertising can weaponize through fear, false urgency, or manufactured hope.
Fear-Based Messaging
Fear appeals are common in health communication, and the evidence on their effectiveness is mixed. A 2021 study found behavioral intention did not significantly differ across threat-only versus coping-focused messaging formats. What isn't ambiguous is the ethical risk: ads that emphasize worst-case scenarios to drive action can cause psychological harm and push patients toward unnecessary treatments. Converting anxiety into appointments is exploitation, not care.
Direct-to-Consumer Pharmaceutical Advertising
The U.S. and New Zealand are the only developed nations that permit DTC prescription drug advertising. The debate around this is not academic. A 2005 JAMA randomized trial found that patient drug requests had a significant effect on physician prescribing in cases of major depression and adjustment disorder. A New Zealand analysis found a terbinafine TV campaign was associated with a doubling of national prescriptions.
Critics argue DTC advertising drives over-prescription, inflates demand for brand-name medications over generics, and expands the boundaries of treatable illness — what researchers call "disease-mongering" — before long-term safety profiles are fully understood.
These commercial pressures compound a third risk area: privacy violations that erode patient trust at the data level.
Privacy Violations in Patient Advertising
HIPAA's protections extend into advertising in ways many marketers don't anticipate. Using before-and-after testimonials, seemingly anonymized case studies, condition-specific online targeting, or retargeting pixels on symptom pages can all constitute protected health information exposure.
The FTC's 2024 enforcement actions make this concrete:
| Company | Penalty | Violation |
|---|---|---|
| GoodRx | $1.5M civil penalty | Shared sensitive health data with third parties for advertising |
| Cerebral | $7M proposed order | Used sensitive data for advertising purposes |
| Monument | $2.5M suspended penalty | Shared alcohol addiction treatment data with Meta and Google |
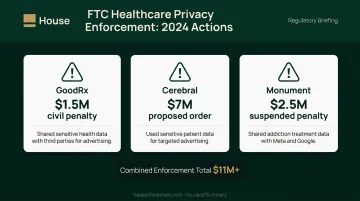
Monument's case is particularly instructive. The FTC alleged the company shared data about users seeking addiction treatment with advertising platforms between 2020 and 2022, despite explicit confidentiality promises to those users. The population was vulnerable, the trust expectation was high, and the breach was severe — a combination that illustrates exactly why regulators are tightening oversight across the sector.
Regulatory and Legal Landmines
Healthcare advertising doesn't answer to one regulator — it answers to several simultaneously:
- FDA (OPDP): Oversees prescription drug and medical device promotion; requires fair balance between benefit and risk disclosure
- FTC: Enforces against unfair or deceptive claims and requires substantiation for all health benefit assertions
- HHS OCR / HIPAA: Governs any use of protected health information, including in advertising contexts
- State medical boards: Set professional conduct standards for physician advertising, which vary significantly by state
This overlap creates genuine complexity. A campaign can be FTC-compliant in its claim structure, FDA-non-compliant in its risk presentation, and simultaneously violate a state board's rules on specialist claims — all at once.
The Digital Privacy Trap
HHS OCR guidance is explicit: HIPAA-regulated entities using online tracking technologies must comply with HIPAA when those tools collect or disclose protected health information. This catches many health systems off guard.
Novant Health agreed to a $6.66 million proposed settlement in 2024 to resolve class-action claims over its use of Meta's tracking pixel on patient portal pages. Legacy Health faces a similar class action (Katherine Layman v. Legacy Health) over alleged patient data disclosure to Meta and Google through pixel tracking.
Pixel placement on authenticated pages, retargeting based on health-related browsing, and audience syncing with ad platforms can all constitute HIPAA violations — even when the ad creative itself is entirely compliant.
Cross-State Exposure
The digital reach that makes online campaigns attractive also multiplies regulatory exposure. A claim permissible under Texas Medical Board guidance may violate California or North Carolina rules, and state boundaries don't disappear just because a campaign runs nationally.
Telehealth advertising adds another layer: most states require providers to be licensed where the patient is located. A national digital campaign can inadvertently promote services in states where the provider has no license to practice.
Platform-Specific Risks: Where Digital Healthcare Ads Go Wrong
Social media and programmatic platforms introduce risks that have nothing to do with ad copy quality. Both Google and Meta operate under strict healthcare advertising policies — Google requires certification for pharmaceutical advertisers and monitors prescription drug keywords; Meta explicitly prohibits ads that "assert or imply personal attributes of the viewer," which rules out targeting based on inferred health conditions.
These aren't edge cases. They're baseline restrictions every healthcare advertiser encounters.
The result is unpredictable campaign performance. Common outcomes include:
- Automated rejection of ads that reference symptoms or medications
- Sudden campaign suspension with no advance warning
- Targeting restrictions that make it difficult to reach patients with relevant conditions
According to eMarketer, According to eMarketer, 52% of consumers across 48 global markets had installed or used an ad blocker as of 2026 — meaning roughly half of web display advertising never reaches its intended audience regardless of content quality.
When platform enforcement lags, the consequences go beyond wasted spend. Reuters reported in 2018 that Google was forced to introduce a vetting process for U.S. drug rehab ads after scammers exploited high-CPC medical keywords to target people seeking addiction treatment — defrauding vulnerable patients before they could reach legitimate care.
Why Newsletter Environments Offer a Different Risk Profile
For healthcare brands navigating these platform restrictions, newsletter-based advertising offers a practical alternative. Placements within the House of Summary network deliver ads directly to subscribers' inboxes, bypassing ad blockers entirely, avoiding algorithmic gatekeeping, and ensuring content adjacency is editorially determined rather than auction-driven.
This matters for healthcare advertisers because programmatic buying can place a pharmaceutical ad next to health misinformation, pseudoscience, or content that directly contradicts the advertiser's clinical claims. Email newsletters with human-written editorial content eliminate that adjacency risk.
How Healthcare Brands Can Advertise More Responsibly
Responsible healthcare advertising is a governance problem first. Most violations aren't intentional — they result from insufficient review before a campaign goes live.
Foundational requirements before any campaign launches:
- Substantiate every claim with current clinical evidence before it appears in any ad format
- Obtain explicit written consent for any patient testimonial, with HIPAA-compliant documentation
- Present risk information fairly — absolute risk alongside relative risk, side effects alongside benefits
- Verify title and credential claims against current licensing board standards in every target state
- Review pixel and tracking setup with a HIPAA-qualified attorney before activating any retargeting

Meeting these requirements narrows your channel choices, too. High-volume, low-context environments — programmatic display, social feeds, search — are harder to control for accuracy and ethical standards than curated editorial formats where content is reviewed before publication.
Pre-campaign legal review by a qualified healthcare attorney isn't optional for healthcare advertisers. The FTC and FDA do not distinguish between deliberate violations and negligent ones when issuing enforcement actions. PhRMA's voluntary DTC advertising principles and the AMA's advertising guidelines (Opinion 9.6.1) both offer frameworks, but professional legal counsel provides the jurisdiction-specific analysis those frameworks cannot.
Frequently Asked Questions
Is healthcare advertising regulated by the government?
Yes, and by multiple agencies simultaneously. The FDA oversees prescription drug and medical device promotion, the FTC enforces against deceptive health claims broadly, HIPAA governs any use of patient data in advertising, and state medical boards regulate professional conduct standards for physician advertising. Compliance requires addressing all four.
What makes healthcare advertising different from other types of advertising?
The audience is often in distress, the product directly affects physical health, and healthcare providers carry professional ethical obligations that go beyond those of standard commercial actors. Misleading an automotive buyer is frustrating; misleading a patient can delay correct treatment.
Can healthcare providers use patient testimonials in their advertising?
Yes, but with significant restrictions. Testimonials must reflect genuine experiences and cannot imply guaranteed outcomes. HIPAA-compliant consent documentation is required, and many jurisdictions prohibit referencing specific clinical outcomes or treatment results. Material connections between the endorser and advertiser must be disclosed clearly.
What are the consequences of violating healthcare advertising regulations?
Consequences range from FTC warning letters and civil penalties to FDA enforcement actions, state licensing board sanctions, civil class-action liability, and criminal prosecution in serious cases. Reputational damage often outlasts the legal proceedings.
Why is direct-to-consumer pharmaceutical advertising so controversial?
The core debate: proponents argue it empowers patients with information about available treatments; critics argue it drives over-prescription of brand-name drugs, inflates patient demand for medications that may not be clinically appropriate, and expands disease categories primarily to grow markets rather than address unmet medical needs.
How can healthcare brands reduce legal risk in advertising?
Engage a qualified healthcare attorney before launch, not after a violation occurs. From there:
- Substantiate all claims with clinical evidence
- Follow FDA and FTC guidelines on risk presentation
- Ensure HIPAA compliance for any data or pixel use
- Choose channels where editorial context is controlled, not algorithmically determined