US healthcare and pharma digital ad spend will reach $24.77 billion in 2025, up 13.3% year-over-year. That's a market too large to approach with guesswork.
This article covers the strategies, compliance considerations, and measurement approaches that separate high-performing healthcare marketing from the noise—written for CMOs, marketing directors, and media buyers who need practical answers, not generic advice.
Key Takeaways
- Health-based audience segmentation outperforms broad demographic targeting when properly de-identified and HIPAA-authorized.
- AI and predictive analytics have moved from experimental to operational priority: 70% of pharma leaders now view AI as an immediate focus.
- HIPAA compliance doesn't block personalization: de-identified data and consented behavioral signals enable relevant messaging without exposing PHI.
- Real healthcare marketing ROI is measured in prescription lift, appointment bookings, and patient retention—not clicks.
- Channel quality beats channel volume: high-attention formats consistently outperform broad-reach placements.
Why Data Has Become Central to Healthcare Marketing Success
Traditional healthcare marketing relied on intuition, broad reach, and hope. TV spots aired to general audiences. Direct mail went to zip codes. Neither approach could tell you whether the right patient saw the right message at the right moment.
Marketers are now building strategies on real-world data (RWD)—a term with a precise regulatory definition. The FDA defines RWD as data relating to patient health status and healthcare delivery routinely collected from sources such as EHRs, claims databases, registries, and digital health technologies. When marketers work with RWD properly, they get a far more accurate picture of the actual patient journey than any survey or focus group can provide.
The Two Audiences That Require Different Data Strategies
Healthcare marketers must reach two fundamentally different audiences:
- Patients (DTC): Motivated by emotion, trust, and accessibility. Need messages that meet them where they are in their care journey—often before they've spoken to a provider.
- Healthcare professionals (HCPs): Motivated by clinical evidence and specialty relevance. Increasingly unreachable through traditional rep visits.
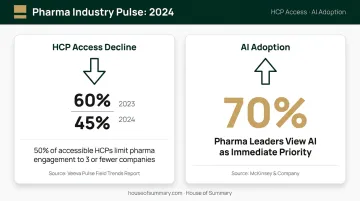
The HCP access problem is severe enough to reshape budgets. Veeva's 2024 field trends data shows US HCP access fell from 60% to 45% between 2023 and 2024, with 50% of accessible HCPs limiting engagement to three or fewer pharma companies. Digital channels have moved from supplementing HCP outreach to serving as its primary path.
Separately, Fierce Pharma reports that 70% of pharma leaders now view AI as an immediate priority—data-driven approaches have moved well past early adoption into standard practice across the industry.
Five Core Data-Driven Strategies Healthcare Marketers Use Today
Audience Segmentation Using Health-Based Data
Healthcare marketers build audience segments using anonymized, de-identified data signals—condition-related codes, treatment patterns, demographic markers, and behavioral indicators like search behavior or content consumption. The critical distinction is between broad demographic targeting (age 45–65, suburban ZIP code) and behavior- or condition-based segmentation (caregivers actively researching a specific treatment, patients who recently searched for specialist referrals).
One important compliance note: condition codes and treatment history are protected health information (PHI) when identifiable. They can support campaign targeting only when properly de-identified under HHS Safe Harbor standards, when the patient has provided authorization, or when a valid HIPAA exception applies. Calling any health-based data "HIPAA-compliant" without that context is legally inaccurate.
Done correctly, segmentation means your DTC campaign reaches patients who are actively considering their options—not everyone in a demographic band who might one day develop a condition.
Predictive Analytics and AI-Powered Targeting
Unlike static audience profiles built on past behavior, AI-powered targeting analyzes engagement history, channel behavior, search patterns, and clinical signals to forecast when a patient or HCP is most likely to engage, what content will resonate, and which channel to use. The result: campaigns reach the right audience before attention drifts, rather than after the moment has passed.
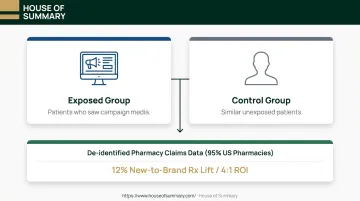
The ROI case is building. An IQVIA measurement study tracking a combined CTV and social campaign against de-identified pharmacy claims data found 12% lift in new-to-brand prescriptions and 4:1 ROI—not from AI alone, but from data-driven campaign orchestration that AI makes possible at scale.
What AI cannot do yet is replace compliance review. Predictive models trained on health data still require the same authorization and de-identification standards as any other PHI-adjacent workflow.
Programmatic Advertising With Healthcare-Grade Precision
Programmatic advertising—automated, real-time ad buying that places messages in front of defined audiences across digital channels—has become a standard execution layer for healthcare campaigns.
In a healthcare context, this means demand-side platforms (DSPs) that support condition-based audience segments, frequency caps, and brand-safety filters aligned with FDA and platform requirements.
Connected TV (CTV) has emerged as a high-performing channel for pharma. The same IQVIA case cited above ran CTV placements alongside social, with prescription lift tracked against real-world pharmacy claims—demonstrating that programmatic reach can be tied to genuine clinical outcomes, not just impressions.
Healthcare and pharma digital ad spend already sits at $24.77 billion in 2025. Programmatic accounts for a substantial share of that display and video spend, and its growth reflects the industry's confidence that automated buying, when governed properly, can deliver precision at scale.
Omnichannel Content Strategy Informed by Behavioral Data
No single channel owns the patient journey. A patient researching a new diagnosis might start on Google, move to a condition-specific website, read their physician's email newsletter, and respond to a social ad before booking an appointment.
HCPs follow a similar multi-touch path—across email, congress platforms, clinical publications, and increasingly, video.
Behavioral data tells you where each audience segment is in that journey. Sequential messaging builds on this:
- Awareness stage — Condition education through programmatic display, search, and broad-reach social
- Consideration stage — Treatment options and provider information via educational content, email, and video
- Decision stage — Targeted follow-up through direct outreach, review platforms, and high-intent search

The key is orchestration. The same message delivered out of sequence loses most of its impact. A patient who just received a diagnosis needs information on what the condition means—not a treatment CTA they're not ready to act on.
Real-World Evidence in Campaign Messaging
Real-world evidence (RWE) is clinical evidence derived from analyzing RWD—actual patient outcomes in real care settings, not controlled trial populations. For HCP marketing, this distinction matters enormously.
Accenture's HCP survey found 59% of HCPs cited technology-driven recommendations based on clinical trial data and real-world data as influential in their treatment decisions. Physicians are skeptical of purely promotional content—they respond to evidence. Campaigns grounded in RWE speak that language.
For DTC audiences, RWE-informed messaging can be translated into patient-relatable proof: "In clinical practice, patients using this treatment reported X outcome." That's more credible than aspirational brand language, and it performs better.
Personalization and Patient Segmentation: Reaching the Right Audience
Building Meaningful Patient Personas
A useful patient persona in healthcare goes well beyond age and income. Clinical context matters: What stage of their condition are they in? Have they already tried one treatment? Are they the patient or the caregiver making the decisions?
Combining EHR-derived insights (when properly de-identified and authorized) with behavioral data from digital platforms — content engagement, search terms, platform preferences — produces personas that reflect real patients rather than guesswork.
The gap between what's possible and what's common is significant: a 2024 AHA/Accenture survey found patients who experience their providers as easy to work with are 84% more likely to remain with those providers. Personalized communication is a direct driver of that experience.
HCP vs. DTC: Why Personalization Looks Different
These two audiences require entirely different approaches:
| Dimension | DTC (Patients) | HCP (Providers) |
|---|---|---|
| Primary motivation | Emotion, trust, accessibility | Clinical evidence, specialty relevance |
| Content format | Plain language, relatable scenarios | Data-supported, peer-level communication |
| Channel priority | Search, social, email, direct mail | Email, clinical platforms, congresses |
| Personalization signal | Journey stage, emotional context | Specialty, prescribing pattern, content preference |
Running the same creative to both audiences doesn't just underperform: it erodes trust with each group for entirely opposite reasons.
The Role of Consent and Preference Data in Personalization
Personalization built on consented data is both a legal requirement and a trust-building practice — patients who feel their privacy is respected are more likely to engage with healthcare messaging and act on it.
This means:
- Collecting explicit consent before any targeted communication
- Offering preference centers where patients and HCPs can control communication frequency and topic
- Using consent management platforms that create auditable records of who agreed to what
Behavioral signals — what content someone engaged with, which searches led them to your site — can power personalization without touching PHI. This approach is both compliant and effective.
Staying Compliant: Navigating HIPAA in Data-Driven Campaigns
HIPAA compliance in marketing isn't just about where data is stored—it governs how patient data can be used in targeting, retargeting, and campaign analytics.
What De-Identification Actually Requires
The HHS Safe Harbor method requires removing 18 specific identifiers before health data can be considered de-identified and used without individual authorization. These include names, geographic data below state level, dates (other than year) directly related to individuals, phone and fax numbers, email addresses, Social Security numbers, medical record numbers, device identifiers, IP addresses, and biometric data.
The financial stakes of getting this wrong are significant. HIPAA Journal's 2026 update reports civil monetary penalties ranging from $145 to $2,190,294 per violation, depending on culpability level. Beyond OCR enforcement, the FTC's 2023 action against GoodRx—resulting in a $1.5 million penalty and a bar on sharing sensitive health data for advertising—shows regulators are targeting health data misuse in digital marketing contexts.
Practical Compliance Safeguards
Those enforcement actions make the operational side hard to ignore. Marketing teams running data-driven campaigns should have these in place:
- Data anonymization protocols aligned with HHS Safe Harbor before any data enters campaign workflows
- Encryption requirements applied to all PHI in transit and at rest
- Vendor vetting to confirm ad platforms, DSPs, and data partners have signed Business Associate Agreements (BAAs) and meet HIPAA standards
- Pixel and tracking technology review—HHS has explicitly stated that tracking technologies like cookies, web beacons, and pixels can implicate HIPAA when they collect PHI from regulated entities' websites
- Regular data flow audits to identify where PHI might enter systems without authorization

Healthcare marketers who onboard third-party data without verifying its provenance are a frequent source of violations. Before integrating any new source, confirm three things: whether it was collected with appropriate consent, how it was de-identified, and whether the provider will sign a BAA. If they won't answer those questions clearly, don't use the data.
Measuring ROI and Choosing the Right Channels
Key Metrics That Reflect True Healthcare Marketing Performance
Clicks and impressions tell you an ad was served. They don't tell you whether it changed behavior.
The metrics that actually matter in healthcare marketing:
- Appointment bookings and form submissions — bottom-of-funnel conversions that indicate genuine patient action
- Prescription lift (NBRx) — for pharma campaigns, the gold standard; IQVIA's methodology links media exposure to de-identified pharmacy claims covering 95% of US pharmacies
- Patient retention rates — long-term indicator of communication quality and trust
- HCP engagement scores — email open rates, content downloads, event attendance, and rep-follow-up rates
- Cost per acquisition (CPA) — compared across channels to identify where budget delivers the most patient or HCP conversions
The 12% new-to-brand prescription lift and 4:1 ROI from the IQVIA CTV/social case is a benchmark worth understanding. It demonstrates that when media exposure is measured against real-world clinical outcomes—not just campaign metrics—healthcare advertising can prove its value in terms that CFOs and brand teams both understand.
Evaluating Channel Performance Against Patient Journey Stages
Channel selection should follow audience intent, not media habit:
- Awareness: Programmatic display, broad-reach social, search
- Consideration: Educational email sequences, video, condition-specific content platforms
- Decision: Targeted direct outreach, review platforms, high-intent search retargeting
Mapping channels to journey stages shifts budget decisions from gut-feel to evidence—rewarding performance rather than volume.
Why Engaged, Targeted Audiences Outperform Broad Reach
Raw audience size is not a proxy for impact. A smaller audience actively seeking health information—one that has opted into relevant content—will consistently outperform a larger audience that was passively interrupted.
Email newsletters make this concrete. Where readers have self-selected, actively open content, and engage without algorithmic interference, the quality of attention is fundamentally different from web display or social feeds. House of Summary's newsletter network, for example, reaches 500,000+ subscribers with over 254,000 daily email opens—giving healthcare advertisers direct inbox access to decision-makers without algorithmic suppression or ad-blocker limitations.
Compliance-friendly formats like native ads and sponsored editorial content fit within healthcare's brand-safety requirements while reaching high-income audiences that map to healthcare's core consumer segments.
Continuous Optimization: Turning Data Into Decisions
Leading healthcare marketing teams treat ROI measurement as an ongoing process. Dashboards and A/B testing frameworks run throughout campaigns, enabling mid-flight spend reallocation based on real performance signals—not end-of-campaign autopsies.
Attribution models in healthcare present a particular challenge—the patient journey spans weeks or months, often across multiple channels. Exposed vs. control measurement designs (matching campaign-exposed populations against similar unexposed groups using de-identified claims data) offer the clearest attribution picture available. It's the same approach IQVIA uses for prescription lift studies, and it's accessible to teams outside large pharma.
Frequently Asked Questions
What is data-driven marketing in healthcare?
Data-driven healthcare marketing uses patient behavioral, demographic, and clinical data to inform, personalize, and measure campaigns—replacing broad-reach approaches with targeted strategies tied to real outcomes. The goal is improving both patient engagement and marketing efficiency simultaneously.
How does HIPAA affect healthcare marketing campaigns?
HIPAA requires de-identification under Safe Harbor standards or explicit patient authorization before health data enters any campaign targeting workflow. Violations carry civil penalties up to $2,190,294 per violation—compliance is an operational necessity, not a checkbox.
What metrics matter most for measuring healthcare marketing ROI?
Focus on appointment bookings, patient acquisition cost, prescription lift, HCP engagement rates, and long-term retention. Clicks and impressions alone don't reflect actual campaign impact.
How is AI being used in healthcare marketing today?
AII builds predictive audience models, personalizes content at scale, optimizes ad placement in real time, and identifies the best channel and timing for each message. It enables healthcare marketers to anticipate patient and HCP needs, not just respond to them.
What channels are most effective for reaching healthcare decision-makers?
Effective channels vary by audience—patients respond to search and social during active research; HCPs engage heavily through email and clinical content platforms. High-engagement formats where audiences have opted in consistently outperform untargeted, interruptive ad placements.
How can healthcare marketers personalize campaigns without violating patient privacy?
Marketers can personalize through de-identified data segments, consented preferences, and behavioral signals like content engagement or search behavior—without touching protected health information. Preference centers and consent management platforms keep this scalable and auditable.